California Department of Public Health (CDPH) and local public health partners are alerting healthcare providers of the emergence of epidemiologically-linked Candida auris (C. auris) cases associated with acute care hospital (ACH), skilled nursing facility (SNF), and outpatient settings in Sacramento and Stanislaus counties since September 2022. Additionally, at the end of January 2023, CDPH was alerted to a case in Contra Costa county associated with an ACH and long-term care setting. These were the first reported C. auris cases in each county, and the patients had no known exposures in healthcare facilities outside of Northern California. These findings suggest there is more transmission in the region than has been identified to date. We continue to see C. auris transmission in Southern California. Patients and residents who have had prolonged admission in healthcare settings, particularly high-acuity care settings including long-term acute care hospitals (LTACH), ventilator-equipped SNF (vSNF), high-acuity ACH units (e.g., intensive care units (ICU) and step-down units (SDU)), are at highest risk of C. auris and other multidrug-resistant organism (MDRO) colonization and infection.
To proactively prevent further spread of C. auris in California, the CDPH Healthcare-Associated Infections (HAI) Program recommends healthcare facilities implement the following updated infection prevention and control (IPC) and containment strategies. A previous recommendation to screen patients from vSNF ventilator units in jurisdictions with known C. auris transmission has been expanded to include screening patients from vSNF ventilator units regardless of geographic location. Recommendations for proactive screening in high-risk facilities are also added.
Active Surveillance
- Assess C. auris status for all patients and residents upon admission, by reviewing medical records and following up with the transferring facility as necessary.
- Conduct screening through colonization testing for persons at highest risk for C. auris, whose status is unknown.
- Screen patients transferring from:
1. any LTACH or vSNF ventilator unit regardless of geographic location;
2. any facility with known C. auris transmission; and
3. any ACH (in addition to any LTACH or vSNF ventilator unit) in Nevada state.
- At LTACHs, screen patients on admission, and conduct routine point prevalence surveys (PPS) per public health guidance.*
- In vSNF ventilator units, conduct routine PPS per public health guidance.*
- Consider screening patients with other known risk factors.†
- If C. auris is identified on admission, notify the transferring facility and local health department of the patient’s status.
- Place all patients screened on admission for C. auris on empiric Contact Precautions while awaiting colonization testing results.‡
Environmental Cleaning and Disinfection
- In LTACHs facility-wide, SNF ventilator units, and ACH high-acuity units (e.g., ICU and SDU), routinely clean and disinfect surfaces and shared medical equipment using an Environmental Protection Agency (EPA)-registered hospital-grade disinfectant effective against C. auris from List P.
- If a List P disinfectant is unavailable, a disinfectant from List K or an appropriately-prepared bleach solution may be used.§
In addition, the CDPH HAI Program continues to recommend the following routine IPC and containment practices for C. auris:
Infection Prevention and Control
- In ACHs and LTACHs, place any patient with C. auris on Contact Precautions, and if possible, in a single room.
- In SNFs, implement Enhanced Standard Precautions facility-wide in the absence of C. auris transmission.
- Consider C. auris and other MDRO status during room placement if and when cohorting patients in a COVID-19 or other respiratory virus isolation area. For example, a patient with both COVID-19 and C.auris can only be placed in the same room as another patient with COVID-19 and C. auris.
- Do NOT reuse or extend use of gloves or gowns.
- Perform hand hygiene before putting on personal protective equipment (PPE), after removing PPE, and before and after patient contact.
- Regularly monitor healthcare personnel (HCP) adherence to IPC practices.
- Continue IPC measures for the duration of a C. auris-colonized or -infected patient’s admission. There is no ‘clearance’ for C. auris colonization.
Routine Surveillance
- Identify all Candida isolates from normally sterile sites to the species level; for Candida isolated from non-sterile sites (e.g., urine), consider species-level identification of isolates from patients at highest risk for C. auris.
- Do not rescreen patients previously identified with C. auris; they can remain colonized indefinitely.
Communication
- Communicate a patient’s C. auris and other MDRO status to any receiving healthcare facility prior to transfer; use an interfacility transfer form.
- Receiving facilities should proactively ask about the patient’s status if not included in the accompanying medical records.
Antimicrobial Stewardship
- Implement antimicrobial stewardship for broad-spectrum antibacterial and antifungal agents to limit the emergence of C. auris, especially multidrug- or pan-resistant C. auris, and other MDROs.
Reporting Requirements
- Report any cases of C. auris and carbapenemase-producing organisms to your local health department, and submit all C. auris isolates identified from a sterile site to a public health laboratory per Title 17.**
- Report other unusual or highly-resistant organisms to your local health department and the CDPH HAI Program at HAIprogram@cdph.ca.gov.
Public Health Testing
- C. auris isolate and colonization testing are available at some local public health laboratories, the CDPH Microbial Diseases Laboratory, and the CDC Antimicrobial Resistance Laboratory Network.
- Contact your local health department to access public health testing services.
Additional Resources
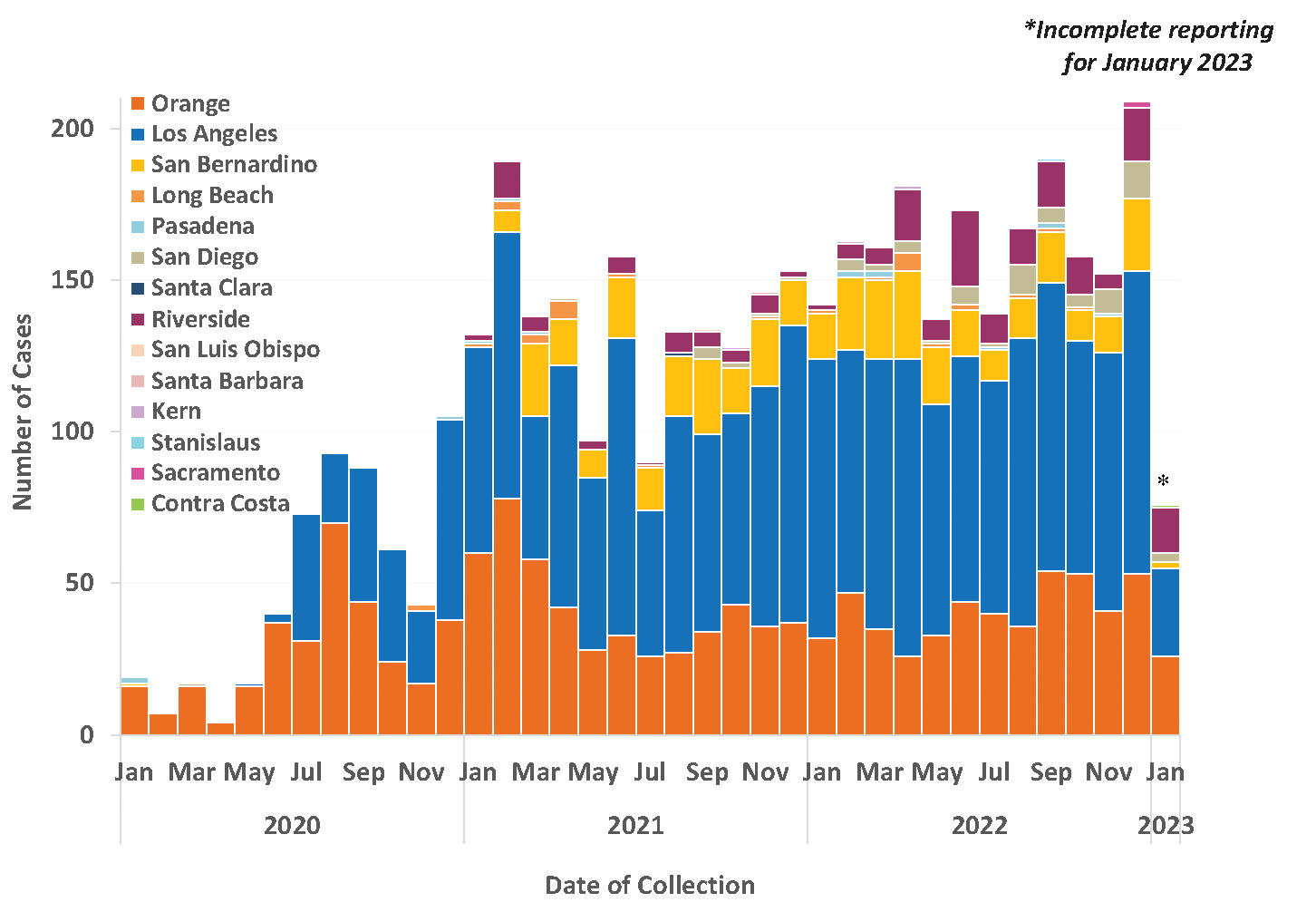
Figure 1. C. auris Cases Reported in California by Local Health Jurisdiction, January 2020–January 2023
‡ As exceptions, if a patient has been screened negative at the transferring facility within 24 hours of transfer, the receiving facility
may opt to not repeat screening on admission. If a patient has a pending screening test collected within 24 hours of admission, the
receiving facility may opt to await those results while placing the patient on empiric Contact Precautions in lieu of rescreening on
admission. If there is any doubt regarding the transferring patient’s screening status, the receiving facility should screen them.
§ Bleach, and List P and List K disinfectants are also effective against SARS-CoV-2.